Thalidomide and the power of the pharmaceutical industry
- Author: H. Sjöström and R. Nilsson
- Publisher: Feltrinelli
- Publication: 31 May 2021
- Pages: 248
This book, published for the first time in January 1973, tells the story of the harmful effects of thalidomide, a drug for pregnant women which proved to be teratogenic: some of the women who had taken it during pregnancy gave birth to phocomelic children, without developed limbs or with other very serious impairments. The authors retrace its entire history, describing the immense power of the pharmaceutical industry, focused solely on economic interests.
This edition, selected by Giulio Maccacaro for Feltrinelli's “Medicina e Power” series, features a preface by Maccacaro himself entitled "And in Italy?" where an interesting analysis of the Italian situation is carried out. These few pages would be enough to make us understand what Italian healthcare institutions were, and are: total subservience to private interests, denial of damage and disinterest in their citizens.
We have decided to offer you Maccacaro's entire preface, containing a brief final focus on the anti-polio vaccine, but our very brief analysis of Maccacaro's text is necessary.
The Sabin anti-polio vaccine, praised by the author of the preface, worked well, so well that it caused and still causes (in the countries of the world where it is still in use) flaccid paralysis from polio.
At the time the risk-benefit analysis was shamelessly in favor of mass vaccination also because, as you will read, if Italy did not collect data on those injured by thalidomide, in your opinion it did so on those affected by the anti-polio vaccine?
Over the years, the Sabin was supplanted by the Salk because the former caused too many problems and adverse reactions and is not used today in the West.
We also remember that currently almost all cases of polio in the world are derived from vaccine viruses, specifically from the Sabin vaccine. The same news that we occasionally hear about tests on wastewater from large cities and the presence of poliovirus refers to "vaccine-derived" strains, i.e. from the secretion, through urine and feces, of portions of the virus by vaccinated subjects. with the "old" Sabin.
It goes without saying that Maccacaro's praise for this vaccine is not shared by Corvelva, but it seemed correct to us to propose the writing in its original version.
The following contents are available only for Corvelva Members. If you are a member, please i login on the site for all content to appear.
A book not to be forgotten (click to open)
This content is reserved for Corvelva Members. If you are a member, click , promising to login.
And in Italy?
“And so, officially speaking, the wolf is as innocent as a lamb.”
Dylan Thomas
Can the eighteen-year-old student who has just enrolled in one of our universities to graduate as a doctor in six years understand the title of this book? Do you know the meaning of “thalidomide”? Imagine the “power of the pharmaceutical industry”? I, his teacher, can answer – in the negative – for him as a mere elementary school student when terms like “thalidomide” and “phocomelia,” names like Chemie Grunenthal and Contergan made headlines around the world.
In fact, the whole world was horrified - over ten years ago - to learn that as a result of a sedative psychotropic drug (thalidomide), administered to women in the first months of pregnancy, thousands of children were born affected by lack of limb development (phocomelia ) or other very serious deformities. That drug had been introduced on the German market, under the name Contergan, by a pharmaceutical company (the Chemie Grunenthal of Stolberg, in Western Germany) who assured and promoted its absolute harmlessness even when its toxic effects were already known.
To increase its profits, the same company had overseen the spread of thalidomide in various other countries, thus spreading the misfortune of children and the desperation of families in each one: 6.000 in West Germany, 400 in Great Britain, 100 in Sweden, and others elsewhere for a total of, according to cautious estimates, between 8.000 and 10.000 cases.
However, such a horrendous catastrophe would have occurred and hidden in the tears of thousands of mothers, each convinced of their own singular misfortune, if some doctors and lawyers had not brought it to light, demonstrating the causes and denouncing their responsibilities. It is to them and to the best part of the foreign press that the thalidomide tragedy has come to an end and has, perhaps, taught us to avoid similar ones. But at the time the medical establishment, accustomed to pleasing the pharmaceutical industry, and its power took sides against them. Chemie Grünenthal left no stone unturned to hide the truth, acquire the silence of those who knew it, intimidate the honesty of those who declared it. His law office even hired a detective to investigate the private lives and political leanings of doctors who had criticized the toxic effects of thalidomide (“Dr. B.'s father,” is written in one of this detective's reports, “ he is a former communist..."). It is right to remember all this to immediately say that the authors of this book are also valiant protagonists of that story.
Henning Sjöström - today a famous lawyer, but the son of farmers, a farmer himself and then a miner while studying for a degree - and Robert Nilsson - a very young and brilliant biochemist from Stockholm University who gave up some years of his career for the cause of children phocomelici - are the two men who led a strenuous battle in Sweden to obtain compensation for the victims of thalidomide. And they won despite the skepticism of their colleagues and the hostility of professional bodies.
Like Sjöström and Nilsson in Sweden, other selfless and courageous doctors and lawyers have fought in Germany, Great Britain and elsewhere for thalidomide children, for their mothers, for their families.
But in Italy? I asked myself this question for the first time when, at the end of last spring, I was told that I was about to receive the manuscript of this book, still unpublished, so that I could evaluate the opportunity of publishing it in the new "Medicine and Power" series of the publishing house Feltrinelli. I posed it to myself and proposed it to others: that is, I conducted a small opinion poll on the topic of "thalidomide", mentioning it - as the occasion arose - to medical colleagues, "pharmaceutical" acquaintances and various friends, including some journalists.
These are the opinions collected and widely shared:
- The thalidomide tragedy belongs, fortunately, to the past: more than ten years now separate us from it;
- it affected many countries, but ours was spared: no Italian cases are known;
- Thalidomide, born in Germany, probably did not come into existence in Italy, that is, it was not produced and sold by our pharmaceutical industry.
Well, none of this is true: as I intend to demonstrate with the help of some data reported by Sjöström and Nilsson and other Italian data discovered in the meantime.
On pages 30-32 of this book the reader finds the list of medicinal specialties based on thalidomide that were sold around 1960 on the European and Canadian markets. It can be summarized, as follows, by nationality:
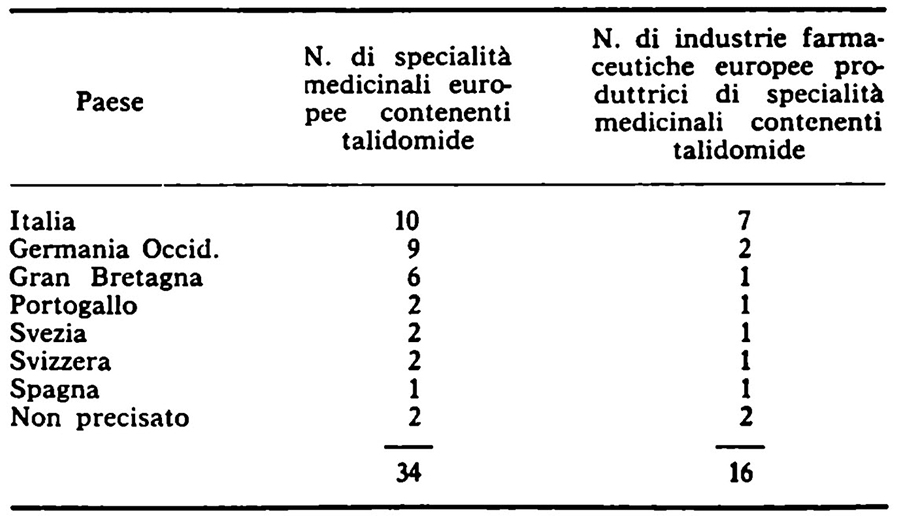
It seems, therefore - scrolling through this list compiled by the American Pharmaceutical Association - that our country has produced 10 out of 34 (about 30%) of the thalidomide medicinal specialties sold in Europe and this is the work of 7 out of 16 (about 44%) of the industries pharmaceutical companies, of various nationalities, engaged in this production.
None of those to whom I communicated this data expressed less than surprise, some incredulity, others put forward the hypothesis that the list contains, for Italy, actually registered names of products that were actually not manufactured: therefore never sold or hired.
However, some verification of this reassuring hypothesis was necessary, aimed at establishing whether the 10 thalidomide specialties were ever actually on the market, that is, sold in Italian pharmacies, and if so: for how long? between which dates?
The answer to these questions is to be found in the pages of "L'informatore pharmaceuticale, Annuario Italiano dei Medicamenti e dei Laboratori" which reached its XXXII edition in 1972: a substantial publication which lists and describes all the medicinal specialties admitted for sale and in trade in Italy, from year to year, indicating its composition, price, manufacturing company, etc. I summarize in the table on p. XI the results of the consultation of the six volumes corresponding to the years from 1958 to 1963.
Note that only the sales and consumption time of each of the specialties listed can be read from the table: not the volume of consumption nor the obviously related volume of production. Given the considerable and even greater interest of these latest data, I conducted research in various places, but without finding any trace of them. There are, it seems, no reporting bodies - state or public - capable of providing such information for those years and for those products. There are, of course, private archives of producers, but their consultation is rather confidential.
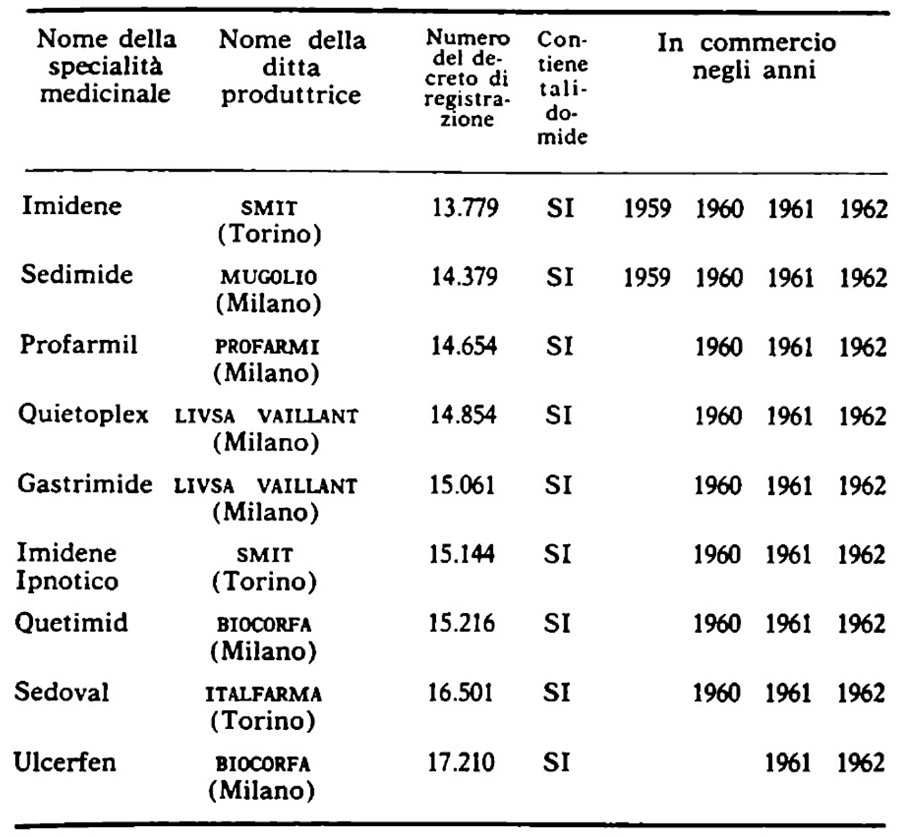
However, it should not be considered too risky to conjecture that SMIT (now UCB-SMIT) of Turin was quite satisfied with its profits when - after having opened the Italian road to thalidomide with Imidene in 1959 - it asked for and obtained authorization to produce and sell a variant aggravated by barbiturates, Hypnotic Imidene, keeping both products on the market until 1962. But, then, the same considerations apply to LIVSA VAILLANT of Milan, which, presenting its Quietoplex in 1960, immediately wanted to combine it with Gastrimide. And also for BIOCORFA, also from Milan, which in the favorable wake traced by its Quetimid and the other seven competing products, believed that it was still worth launching a ninth, Ulcerfen, in 1961, when they were already starting to race for the world news on the toxic effects of thalidomide.
What to think, then? At this point of my little research - and my big surprise - I had in front of me nine thalidomide specialties, demonstrably sold in Italy between 1959 and 1962, and at least as many assurances that there had been no cases of thalidomide phocomelia in Italy.
Since the first term of the contradiction was now established as a fact, all that remained was to doubt the second. Especially after a short sentence on page 127 of this book told me what I had not learned from others:
Despite the occurrence of cases of phocomelia in Turin in June 1962, some of these products were only recalled in Italy in September 1962.
Not one more indication, but three friends - a child care worker, an anatomic pathologist and a journalist - helped me immediately follow this trail to its origin. On 15 June 1962, professors Maria Gomirato-Sandrucci, director of the Institute of Childcare, and Ruggero Ceppellini, director of the Institute of Medical Genetics of the University of Turin, read a communication at the Academy of Medicine of the same city during the which they declared:
In our series of past years there has been no shortage of cases of amelia and phocomelia which have come to our attention at the rate of one case every two years. Given this rarity, we were struck by the fact that in just over a month (from 7 April to 16 May of this year), as many as five amelic and phocomelic newborns from Turin and outside Turin were admitted to the Immature Center of our Clinic. .
Six months later the same authors published a more extensive and detailed report on the same cases which in the meantime had risen to 7. At the conclusion of a documented and careful examination of all the possible causes that could have explained such an exceptional frequency of such a rare congenital malformation, Gomirato-Sandrucci and Ceppellini dictate these lines which deserve to be transcribed and meditated on:
It turned out that 4 mothers had definitely introduced a medicine based on n-phthalyl glutamic acid imide. The safety of this administration derives both from the spontaneous admission of the name of the drug by the woman, and from having recognized the bottle among many others, and finally from the confirmation of the doctor who had prescribed the drug. In all cases it was the same commercial tablet package containing 50 mg of n-phthalyl-glutamic acid imide each. In a fifth case we were not able to have absolute certainty regarding the administration of the medicine as the woman certainly introduced some sedative tablets of which she does not remember the name between the first and second month of pregnancy and also the attending physician is rather uncertain about the possible prescription of a medicine based on n-phthalyl glutamic acid imide. In the other two cases (1 and 2) the introduction of the medicine in question was decidedly denied by both the mothers and the treating doctors.
In these lines the name "thalidomide" never occurs but its chemical version in full, "n-phthalyl-glutamic acid imide", unknown to the public, to the general practitioner and also to the specialist dedicated above all to professional practice. For all of them the only significant and memorable names are those of the specialties (Imidene, Sedimide, Profarmil, etc.) which refer to the names of the respective manufacturing industries (SMIT, MUGOLIO, PROFARMI, etc.) but there is no trace of them in the report by the two scholars from Turin. From this report (published on 3 November 1962) we also learn that, of the four children whose mother had certainly taken thalidomide in the first months of pregnancy, two were alive at the date of writing of the text: of one, Antonella B., born on 3 opened in 1962 by a worker and a housewife, and perfectly formed except for the total lack of arms, it is said:
Course: the little girl has always enjoyed good health and has shown regular, satisfactory growth. She is currently hospitalized in good health at a healthcare institution.
Of the other, Renato A., born on 7 August 1962 to a worker and a housewife, with serious deformations in all four limbs, but normal as regards the vital organs, it is said:
Course: the child did not present any symptoms attributable to any other malformations other than those reported in the limbs. The growth was rather slow but regular. The child is still hospitalized in our institute and still has a notable weight deficit compared to normal.
What happens to Renato and Antonella today? I don't know, but I'm asking. Just as I didn't know and I asked myself - at this point in a research that took me from surprise to surprise but also from anguish to anguish - whether the limited Turin epidemic of thalidomide malformations was, as it seemed from reading the texts cited, truly the the only one that occurred in Italy; or if other children were born horribly mutilated and deformed, as a result of the evil drug, also elsewhere: where, then, and how many?
In an attempt to find an answer to these questions, I wrote, two months ago, to over a hundred colleagues, holders of chairs in the various Italian medical faculties such as: obstetrics and gynaecology, paediatrics, childcare, pharmacology and others having scientific and practical relevance with the problem of thalidomide phocomelia. I simply asked each of them to report to me, if he had knowledge of them, data and cases of affected children.
Thirty-five colleagues, to whom I renew my thanks here, responded from different parts of Italy: most to tell me that they had never heard of any cases of thalidomide phocomelia having occurred in Italy, some to inform me of the observations of the two Turin scholars already mentioned, others still to give me directions that I didn't know.
Among the latter emerges, because it collects others, a review, compiled in collaboration,(6) by Professor Cesare Torricelli, director of the Provincial Institute for Child Protection and Assistance of Milan, who begins thus:
In April 1963, nine months had passed since the withdrawal of Thalidomide-based preparations from the market. In this review we therefore aim to expose on the topic of congenital malformations attributed to Thalidomide the notions drawn from the experience of most of the Authors and from our direct observation.
Torricelli, in fact, before describing the cases he directly studied, informs us of others of "certain thalidomide etiology," that is, certainly caused by one of those specialties - unfortunately never mentioned in relation to the individual cases - that I have listed in the table: one in Syracuse and one in Palermo, one in Portici (Naples), one in Modena, one in Rome, one in Busseto (Parma), one in Massalombarda (Ravenna), one in Sassuolo (Modena), two others in Turin, one in Alessandria, one in Mestre, one in Pavia.
The mention of these cases is followed by the description of nineteen others who arrived at the Milanese Institute from the city and surrounding areas; for eleven of them... The use of thalidomide preparations always taken within the first three months of pregnancy has been safely demonstrated.
For the other cases this use is not documented with sufficient certainty, but nor excluded: "it is worthy of note," the authors underline,
that even in all these latter cases the sympathetic disturbances in the first months of pregnancy had been particularly intense and that the mothers had used numerous preparations, especially "sedatives."
Torricelli concludes his review by stating that in Italy
the number of malformed births of suspected thalidomide etiology was small: 50 cases, of which 27 with proven etiology, 11 of which in Milan.
But everything leads us to believe that this estimate can only be wrong by default. In fact, Torricelli himself notes:
[these] are the figures that we collected directly as we did not receive any response from the Ministry of Health we consulted.
Nor does it appear, after ten years, that the Ministry itself has ever published a report on the disastrous event. It must also be said that Torricelli's review, despite being the most extensive to appear in Italy, does not include any reports - perhaps because they emerged later or in particular locations - of other confirmed cases. Finally, it is worth noting the singular concentration of cases in just two cities, Milan and Turin, which is matched by the absence of cases in other centers of comparable demographic size and the peripheral and sporadic dissemination of individual others. What to think, then, of these epidemic outbreaks in the Piedmontese and Lombardy capitals? Real or apparent? How to interpret them in one case and how in the other? A reevaluation of the statistical dimensions of the phenomenon may depend on the answer to these questions.
If it really was a greater incidence of thalidomide phocomelia in the two subalpine cities, we can only assume there was a greater prescription of the drug in general and to pregnant women in particular. But this explanation would require another - for example, on the behavior of doctors and pharmacists - which I cannot see unless I attribute some meaning to Turin being home to SMIT, the pharmaceutical industry which opened the Italian border to thalidomide, and Milan is home to four other pharmaceutical companies that immediately launched themselves in pursuit of SMIT and its thalidomide profits.
Indeed, these circumstances can suggest a greater and more persuasive propagandistic presence of the producers among the clinicians and doctors of the respective cities and provinces: those who know about these things and know certain local therapeutic fashions, otherwise inexplicable, cannot easily dismiss this hypothesis. But he also knows that the advertising permeation (which corresponds to at least 30% of the price of a drug) of which the pharmaceutical industry is capable soon goes beyond local or regional borders to persuasively reach even the most distant doctors. Therefore a drug which, it seems, arrives and harms Syracuse but not Bari, Sassuolo but not Bologna, Mestre but not Padua - to focus on cases in Turin and Milan - leaves some unresolved perplexities.
Which leads us to reflect on the other possibility envisaged above: perhaps the exceptional nature of the outbreaks in Turin and Milan is only apparent, in the sense that particular conditions would have existed in the two cities not for the ignition of the two small epidemics but for the necessary attention to their relief. Elsewhere, less or less prepared attention would not have grasped a phenomenon of the same size or would not have interpreted its causes correctly. The surprising observation that a large number of qualified colleagues believe and respond, even today, to have no recollection of cases or knowledge of scientific works from which it appears that thalidomide phocomelia has occurred and is repeated in Italy also fits well with this conjecture. . On the other hand, it is the same scholars from Turin and Milan who inform us how singular circumstances, probably not known to others, had attracted and stimulated their medical and scientific interest in the problem: those who had already been dedicated to related research for some time and these (10 ) fervently intent on preparing a very demanding congressional report on the same topic!
I therefore advance the reasonable hypothesis that in the Piedmontese and Lombardy capitals cases of thalidomide malformation have been recognized but have not occurred more than elsewhere; that is, I am inclined to believe that elsewhere as many cases have occurred, in relation to the number of births, but fewer have been recognised.
Note that the object of recognition is not - better: it would not have been, then - phocomelia or other congenital malformation as such, because the very serious ones we are talking about here are evident even to the eye of a midwife: it is - better: it should have been - the relationship between the malformation and the use of thalidomide in the first months of pregnancy. A report that, in order to be identified, if it existed, would have required some things. In doctors who had the opportunity: adequate information on the problem, the ability to investigate it, the will to solve it. In mothers who had had the misfortune: the memory of the drugs taken during pregnancy, the de visu demonstration of all those accused, a frank explanation on the meaning of the investigation. I do not believe that these conditions always or even often occurred where a child phocomelic from thalidomide was born: however, the non-compliance of just one was enough to remove that child from the list of victims forever.
In fact, if the frequency of thalidomide malformations in the Italian population were estimated overall at the level of just one case per 10.000 births for the three-year period 1960-1962, 95 new cases would have been produced but not necessarily recognised, for each of the same years, instead of the 50 in total reported by Torricelli. Naturally, no verification is possible today, but only an observation: congenital deformations of the locomotor system and in particular congenital aplasia of the limbs show a sudden marked increase in numbers on a national scale (respectively of hundreds and tens of cases per year) precisely starting from 1961, as in the other countries affected by the thalidomide tragedy.
It is, therefore, not true - to return to the results of the initial survey: corresponding, as I further verified, to a significantly acquittal erroneous belief, very widespread in public opinion and even in the large majority of medical opinion - it is not, therefore, it is true that the Italian pharmaceutical industry has not produced and marketed, in various forms and under different names, the harmful thalidomide.
Above all, it is not true that our country has not been hit by the scourge of phocomelia and other malformations resulting from taking that drug.
And finally it is not true, indeed it is probably far from reality, that in Italy in total there are just over 20 cases, a figure fortunately much lower than the approximately 10.000 cases which would represent the total number of cases observed throughout the world.
It is certain that the phenomenon did not have the same dimensions in us as in West Germany and it is probable that it remained below those in Great Britain; but nothing excludes the possibility of comparing its absolute values to those of Sweden where the Swedish Medical Association estimated that approximately 150 children were harmed by thalidomide, of which 6 out of 10 died and the others survived.
It is at this point, at the point where the further life of these four children is decided, that the Italian picture becomes distressingly dark. To realize this, it is no longer necessary to think in statistical terms: especially if the human identity of individual cases can be lost among these apparently comforting terms. Instead, let us stick strictly to the published data and decide to believe that no others exist and have not existed.
But the question already asked remains and is renewed: what happened to Antonella B. and Renato A., the surviving children of Turin? What happened to Giuseppina R., Giorgio P., Giuseppina F., Maria V., Patrizia D. and Giuseppina G., the surviving children of Milan?
Some of them without arms, others without legs, one without all four limbs: disappeared now? And then we must ask and have the right to know why all the Italian thalidomide children died, while 40% of the English, Swedish and German ones are still living and growing. Or they are alive and then you have to ask and have the right to know how and where their existence takes place, who takes care of them and in what way, who provides for their enormous needs and to what extent, who accompanies them and assists them in this even more terrible phase of their life: entering adolescence? Because for them the tragedy of thalidomide does not belong to the past, but lives and grows with them, becoming - with every new day, at every other age - more cruel and definitive. For so much offense, for so much pain there is no possible repair or adequate compensation. No human destitution allows for venal restitution. But it imposes, on those who bear objective responsibility, at least the duty to mitigate the consequences by every means and measure.
In Sweden - above all thanks to Sjöström and Nilsson, but also to vigorous pressure exerted by the press and public opinion - the Astra Company, an industry producing medicinal specialties containing thalidomide, was induced to pay, for every child affected by effects of the drug, the annual income corresponding, net of inflation, to a capital of 150 million lire.
In Great Britain, the Distillers Co. Ltd., after having signed a similar commitment, albeit for a smaller compensation, and having tried every technicality to avoid honoring it, has been hit in the last two months by a press campaign (which was followed a parliamentary initiative and the boycott of its products by English students) developed following the publication of this book by the Penguin Books publishing house. Therefore the managers of Distillers Co. Ltd. were forced to make greater commitments for the provision of funds to children affected by thalidomide: their last proposal of which I am informed (14 December 1972) amounts to 17 billion lire equal to to an invested capital of 50 million for each child. But a group of deputies, from the majority and the minority together, is working to obtain double this amount in order to guarantee to the little phocomelic patients what is indispensable (prostheses to be changed from year to year, means of locomotion, assistance, etc.) to alleviate at least partly the pain of their existence.
In West Germany, Chemie Grünenthal had to appear in a trial - the longest, as the reader will learn in this book, after the Nuremberg trial of the Nazi criminals - of which she tried in every way to avoid the conclusion and the sentence, finally reaching to the commitment - contracted, not yet kept, but certainly no longer declineable - to pay 21 billion lire for German phocomelic children. All this, let us be clear, is not enough to restore what was taken from the life of a single child nor to grant absolution to the responsibility of an entire system.
But in Italy, not even this was done, none of this happened. Here it is not even known whether "thalidomide" children ever existed and whether they still survive. Here the rare publications that talk about it are written for conferences and scientific journals. Here we never say, even if we know exactly, which mother took which product. Here, in any case, the name of the producing industries is always kept silent. Here no health authority promotes an ad hoc investigation and publishes its results. Here, above all, no one seems to have asked the six pharmaceutical sisters to take financial responsibility for those eight children: 1,3 children each.
But, perhaps, an Italian phocomelic child is worth less or suffers less than his Swedish, English and German companion. Or, he is worth nothing and no longer suffers. Or, perhaps, the case of him and the other seven, if it had become public, would have brought to light the story of others. How many others? And perhaps, then, the industries involved and the pharmaceutical world would have suffered too much and would have been sorry. And this, in Italy, would in turn have created so many other sorrows that eight children, even if phocomelic, could not even imagine them.
Am I suggesting that the interweaving of relationships between the pharmaceutical industry, healthcare administration and the medical profession is, in our country, so dense as to disappoint any attempt to look at it transparently? Perhaps so, but beyond this opaque thickness I see, and am struck by, these dates: thalidomide was withdrawn from sale to the public in West Germany, Sweden and Great Britain between the last ten days of November and the first of December 1961. But our Minister of Health, who was informed of it, did not suspend, even as a precaution, the sale of Italian medicinal specialties containing the evil drug until the summer of 1962. What did it mean for him and for the other interested parties this incredible delay, I don't know. I know that for Giuseppina G., who was born in Milan on 14 September 1962 to a mother treated with thalidomide during the first two months of pregnancy, that is, from mid-January to mid-March 1962, being Italian meant above all this: being born with an atypical phocomelia of the lower and upper limbs.
But already the year before, the Minister of Health had allowed himself - calling for prudence! - another delay, intended to please a certain pharmaceutical industry, which cost the lives of many children as well as the paralysis of many others. This very serious complaint, made publicly by the Collective of the Istituto Superiore di Sanità, has never been denied. It is a bruising story, extremely significant, which must be known.
I take the following data from a recent report by the World Health Organization.
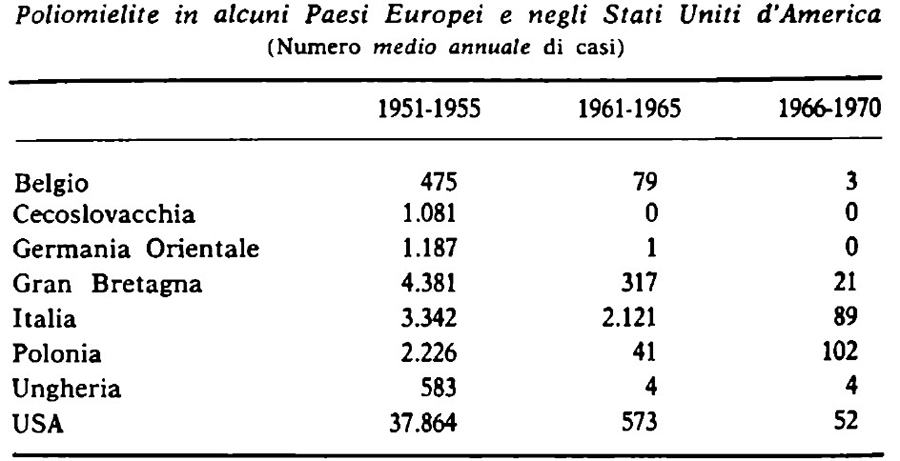
It is clear, from a simple look at the figures, that in Italy polio continued to claim thousands of victims even in the five-year period in which it had already been defeated and even eradicated in other countries. To understand how this could have happened, we must remember that in the 10s the first vaccines against the terrible disease were proposed and tested: credit for the first goes to J. Salk who developed a vaccine made up of killed viruses, which can be administered by injection; for the second to A. Sabin who prepared a vaccine consisting of attenuated viruses, which could be administered orally. Extensive trials clearly demonstrated that the second vaccine is much more effective than the first in protecting those who receive it, and in particular children, against polio which - remember - is lethal in about XNUMX% of cases and paralyzing in the others.
This superiority of the oral vaccine and its positive use in very large populations were already known in the summer of 1960: it was widely discussed during the International Conference on Polio (18) held in Copenhagen in July of that year. Two months later, on 30 September, Professor Sabin himself read in Rome - right in the classroom of that Istituto Superiore di Sanità which is the technical-scientific farmyard of the Ministry of the same name - a report entitled "Results obtained in different parts of the world in mass vaccination with live polio vaccine”. This report fully confirmed the positive data of which the international medical world had already been informed, it stated that mass oral vaccination had already been carried out in 1959 in Czechoslovakia and in 1960 in East Germany, Poland and Hungary; he added that in 1960 over 70 million people were already vaccinated in the USSR with the oral vaccine and that they would become 198 million in 1961; it announced mass vaccination in the USA for the following year where in fact it was carried out in March 1961, as well as in 1962 in Belgium and Great Britain.
Our Minister of Health knew these things and on the other hand he knew that, although the Salk vaccine had begun to be distributed to the Italian population in 1958, our country still counted, in 1959 alone, 4.110 new cases of polio, of which 630 deaths; 3.555 cases, of which 451 deaths, would have been the corresponding figures for 1960. He was therefore able to reach decisions that other rulers had already taken; he was urged to do so by the urgency and epidemiological dimensions of the problem in Italy; he was comforted by the authoritative opinion of doctors, technicians and scientists.
But what happened instead? Sabin's conference, the typed text of which still exists in Rome, was never published, against all custom and despite its importance. However, the speech that the Minister of Health addressed to the Italian pediatricians gathered in the capital a few days later is published:
...speaking today before such an elected assembly of specialists in a branch of medical science which concerns early childhood, the one most subject to the polio disease, I believe it is right to remember, as the sole and direct person responsible for the protection of public health, that Polio vaccination with live vaccine will not be authorized in Italy for now. The Ministry of Health cannot make Italian children experimental guinea pigs, as they actually would be, given the still experimental phase of the live vaccine. Consequently, the live vaccine will not be registered in our country for the time being, nor will its manufacture be authorized for export purposes.
The prudence of the minister, or rather of two ministers, is amply demonstrated by the fact that they waited until 1964 before starting the new vaccination: that "now" and that "moment" thus lasted three years during which 9.509 occurred in Italy cases of polio: 1.078 died and 8.431 remained paralyzed.
The reader now has a statistical understanding of the data contained in the recent World Health Organization report and which I have reproduced on p. XXIII. But for a political understanding of them it may not be useless to know other facts.
In the autumn of 1960, when A. Sabin came to the Istituto Superiore di Sanità and the Minister of Health went to the Pediatric Congress, the production of the anti-polio vaccine was reserved for two pharmaceutical industries: the ISI (Italian Serotherapy Institute) of Naples and the ISM (Milan Serotherapy Institute) in Milan. The third Italian industry specialized in the "serums and vaccines" sector is SCLAVO (Istituto Sieroterapico Vaccinogeno Toscano) of Siena which, at that time, was also preparing to produce an anti-polio vaccine, but precisely of the Sabin type.
Instead, the ISI and the ISM were already producing, and only, Salk-type vaccine: they had equipped the plants for it, they were filling the warehouses with it. Italian production was duopolistic and the market was practically monopsonic since one buyer largely dominated the others: the Ministry of Health itself. It is this Ministry that, when it received news that SCLAVO had prepared an oral Sabin-type vaccine, sent a provincial doctor to seal the bottles to prevent its distribution. Meanwhile, the production and sales, the depreciation of the plants, the depletion of inventories and the accumulation of profits of the ISI and ISM continued. This is how we arrive at 1964 when another Minister of Health, also convinced, but fortunately in a different sense, that his ministry "cannot make Italian children experimental guinea pigs," started the distribution of the attenuated oral vaccine. . Since then, polio has practically disappeared: 20 cases throughout Italy during the first nine months of 1971!
We can, therefore, conclude that the vast majority of the 9.509 cases of polio that occurred in Italy in the three-year period 1961-1963 could have been spared - to understand what this means we need to make the effort to think about them one by one, family by family, child by child , coffin for coffin, paralysis for paralysis - if a certain vaccine had been promptly replaced by another. But the enjoyment of this benefit was postponed by subordinating it to precise amortization calculations... because the profit needs of the industry that had until then produced the Salk vaccine corresponded to a total subservience of the state bodies and their highest responsible, the Minister of Healthcare.
These two Italian events - on which we would like others to shed more light and obtain some reparations - are, in fact, only one: they present the same protagonists, involve the same responsibilities, point to the same dangers.
Above all, they resolve themselves together in the irreparable and still uncompensated suffering of unknown and even outcast victims.
They are contemporary and coherent events also in their apparent autonomy and contradictory nature: in one case, that of thalidomide, free sale was allowed - beyond all reasonable limits - to an evil drug while waiting for mothers and children to become guinea pigs and victims to demonstrate its toxicity although already known; in the other, that of polio, a beneficial vaccine was prevented from being produced and distributed in order to prevent mothers and children from becoming guinea pigs and victims of its equally well-known... harmlessness.
But contradictions like these usually don't stand up to the test of a simple question: who got the sacrifice each time and who got the advantage? Well, here - that is, in one case and in the other - it seems to me no doubt that public health has been sacrificed to the advantage of private capital, that man's pain and infirmity have been paid to greed and arrogance of a power: that of the pharmaceutical industry.
This power is the true underlying theme of Sjöström and Nilsson's book who tell us about it from page to page, albeit in the manner of a true and anguished story. Adhering to the same choice, this introductory note also wanted to concentrate on the story and comparison of two Italian experiences: above all so that the reader is not led to believe - as is often wanted of him - that "these things" are from other places and 'another time.
But it will be convenient to point out to the reader himself that the power of the pharmaceutical industry is too complex and articulated, relevant and incidental, for us to be satisfied with recognizing it and judging it in its most sensational manifestations.
It will therefore be necessary to go further: in the structural analysis of this power, of its relationships with the political one, of its connection with the medical one. It will be necessary to identify its position in the healthcare city, its irradiation in the healthcare system, its pre-emption on scientific activity.
The political role of the drug itself will have to be analysed: how it serves the doctor and how the doctor serves it, for the service that both must render; what image of himself he proposes to the patient and how he himself distorts the image of himself; how it adapts to every need for social management and how it suggests, to the point of dictating, the most repressive models.
This series already has other titles for an in-depth exploration of these themes.
Giulio A. Maccacaro
January 1973