Measles: what parents need to know
Corvelva Staff
Illnesses
What is measles?
from: www.physiciansforinformedconsent.org
Measles is a self-limiting childhood viral infection.
- Symptoms of measles include a prodromal (early) phase that involves coughing, runny nose, eye irritation and fever, followed by general waves of illness that
they last from 4 to 10 days.1 - Measles is contagious during the prodromal phase and 3-4 days after the onset phase.1
- Many measles cases are benign and are not reported to the public health departments.2
- Before the introduction of the mass vaccination program against measles, almost everyone contracted measles within 15 years and strengthened the immune system.1
- In rare situations, measles can cause brain damage and death.3-4
The CDC have published fatal cases of measles based on those reported. However, about 90% of measles cases are benign and are not reported to the CDC.2 By calculating the percentages of fatality cases on the basis of the reported cases (which constitute only 10%), we obtain a percentage of cases is 10 times higher than the current one of the general population. The analysis of the data here is based on the total of measles cases (those reported and those not reported).
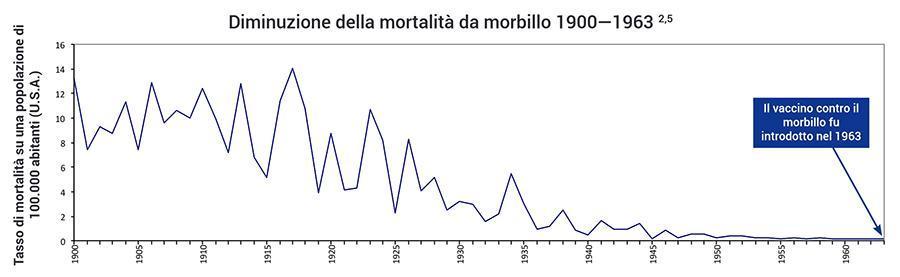
Figure 1: Measles deaths decreased 98% from 1900 to 1963 before the introduction of the vaccine.
What are the risks?
In the modern age, it is rare to suffer from permanent disabilities or death from measles in the United States. Between 1900 and 1963, the mortality rate from measles dropped from 13,3 per 100.000 to 0,2 per 100,000 among the population due to improved living conditions, nutrition and medical care - a decrease 98% (Fig. 1).2-5 Malnutrition, especially vitamin A deficiency, is the leading cause of around 90.000 measles deaths per year in underdeveloped countries.6 In the United States and other developed countries, 75–92% of hospitalized measles cases have low vitamin A intake.7-8
Measles and national research studies have documented the following:
- 1 in 10.000 (0,01%) cases of measles can be fatal. 3
- 3 to 3,5 in 10.000 cases (0,03% to 0,035%) of measles end in convulsions.9
- 1 in 20.000 cases (0.005%) of measles end in encephalitis.4
- 1 in 80.000 cases (0.00125%) end up in a permanent measles encephalitis disability.4
- 7 out of 1.000 cases (0,7%) are hospitalized.10
- 6 to 22 out of 1.000.000 cases (0,0006–0,0022%) of measles end in subacute sclerosing panencephalitis (SSPE).11
3. What types of measles treatments are available?
Since measles disappears on its own in most cases, only supportive treatments are usually needed. Therefore, the following treatments are considered:
- Rest
- Hydration
- High dose of vitamin A12
- Immunoglobulin (available for patients with compromised immune systems, such as those who are undergoing chemotherapy)13
The World Health Organization (WHO) recommended to treat many serious cases of measles with a high dose of vitamin A, 50.000–200.000 IU, per orally for two consecutive days.13
Are there any benefits to getting measles?
Some studies suggest that there is a relationship between naturally contracted measles infection and a reduced risk of Hodgkin and non-Hodgkin lymphomas, as well as a reduced risk of topical diseases such as hay fever, eczema and asthma.14-18 In addition, measles infections are associated with lower risk of cardiovascular disease mortality in adulthood.19 On the other hand, new born babies
mothers who naturally contracted measles are protected from contracting measles thanks to the mother's immunity for longer than infants born to vaccinated mothers.20
The measles vaccine?
The measles vaccine was introduced in the USA in 1963 but is only available today as part of the measles, mumps and rubella (MPR) vaccine. This significantly reduced the incidence of measles. However, the vaccine cannot prevent all measles cases, as reported by bankruptcy cases.21 The pharmaceutical company package insert contains information about the ingredients contained in the vaccine, the side effects and the vaccine ratings. For example, "the MPR II vaccine has not been evaluated for its potential carcinogenic or mutagenic risks or that impair fertility."11 Furthermore, it has not been proven that the risks of permanent damage and death from MPR vaccine are lower than those caused by measles (Fig. 2).22-23
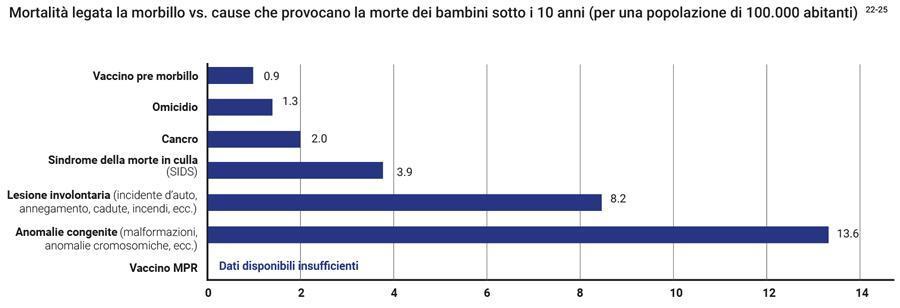
Figure 2: The graph shows the rate of death from measles before the introduction of the vaccine, when measles was a common viral infection in children, and compares it with the causes that cause death in children under 10 today. Therefore, in the pre-vaccine stage, the measles death rate per 100.000 was 0,9 for children under 10 years. In 2015, the death rate per 100.000 per murder was
of 1,3, followed by cancer (2,0), SIDS (3,9), unintentional damage (8,2), and congenital anomalies (13,6). The rate of death or permanent damage from MPR vaccines is unknown as the research studies available are unable to establish it with sufficient accuracy.22-23
These prospectuses are for informational use only and should not be used as medical advice.
References
- Centers for Disease Control. Epidemiology and prevention of vaccine-preventable diseases. 13th ed. Hamborsky J, Kroger
A, Wolfe S, editors. Washington DC: Public Health Foundation; 2015. 209-15. - Between 1959 and 1962, annually there were about 4 million cases, of which 440,000 (11%) were reported.
• Centers for Disease Control. Epidemiology and prevention of vaccine-preventable diseases. 13th ed. Hamborsky J, Kroger A, Wolfe S, editors. Washington DC: Public Health Foundation; 2015. Appendix E3.
• Centers for Disease Control. Measles prevention: recommendations of the Immunization Practices Advisory Committee (ACIP). Morbidity and Mortality Weekly Report. 1989; 38 (S-9): 1. - Between 1959 and 1962, annually there were 400 measles deaths out of 4 million cases, about 1 in 10,000 cases.
• Same sources as reference 2.
• Langmuir AD, Henderson DA, Serfling RE, Sherman IL. The importance of measles as a health problem. Am J Public Health Nations Health. 1962 Feb; 52 (2) Suppl: 1-4. - Measles surveillance in the 1980s and 1990s showed that there are half as many cases of measles encephalitis as there are measles deaths, 1 in 20,000 cases (50% of 1 in 10,000 cases of death). Of these cases, 25% (1 in 80,000 cases) result in residual neurological injury.
Same sources as references 1 and 3. - Grove RD; Hetzel AM; US Department of Health, Education, and Welfare. Vital statistic rates in the United States 1940-1960. Washington DC: US Government Printing Office; 1968. 559-603.
- The measles case-fatality rate in underdeveloped nations, where vitamin A deficiency is prevalent, is about 3–6% of reported cases, 30 to 60 times higher than in developed countries.
• World Health Organization. Measles: fact sheet [updated 2017 Oct; cited 2017 Dec 7]. http://www.who.int/mediacentre/factsheets/fs286/en. - Butler JC, Havens PL, Sowell AL, Huff DL, Peterson DE, Day SE, Chusid MJ, Bennin RA, Circo R, Davis JP. Measles severity and serum retinol (vitamin A) concentration among children in the United States. Pediatrics. 1993 Jun; 91 (6): 1177-81.
- Hussey GD, Klein M. A randomized, controlled trial of vitamin A in children with severe measles. N Engl J Med. 1990 July; 323 (3): 160-4.
- Measles surveillance in the 1980s and 1990s showed that there are 3 to 3.5 times more measles seizures than measles deaths (3 to 3.5 for 10,000 cases).
Same sources as references 1 and 3. - Measles surveillance in the 1980s and 1990s showed that there are about 70 times more measles hospitalizations than measles deaths (7 per 1,000 cases).
• Same sources as reference 3.
• Centers for Disease Control. Current trends measles - United States, 1989 and first 20 weeks 1990, June 1990. MMWR. 1990; 39 (21): 353-5,361-3. - US Food and Drug Administration: MMR II (measles, mumps, and rubella virus vaccine live). Whitehouse Station: Merck & Co., Inc .; c1971 [cited 2017 June 21]. https://www.fda.gov/downloads/biologicsbloodvaccines/vaccines/approvedproduct/ucm123789.pdf.
- Perry RT, Halsey NA. The clinical significance of measles: a review. J Infect Dis. 2004 May 1; 189 Suppl 1: S4-16.
- California Department of Public Health. Measles investigation Quicksheet. May 2011.
- Alexander FE, Jarrett RF, Lawrence D, Armstrong AA, Freeland J, Gokhale DA, Kane E, Taylor GM, Wright DH, Cartwright RA. Risk factors for Hodgkin's disease by Epstein-Barr virus (EBV) status: prior infection by EBV and other agents. Br J Cancer. 2000 Mar; 82 (5): 1117-21.
- Glaser SL, Keegan TH, Clarke CA, Trinh M, Dorfman RF, Mann RB, DiGiuseppe JA, Ambinder RF. Exposure to childhood infections and risk of Epstein-Barr virus — defined Hodgkin's lymphoma in
women. Int J Cancer. 2005 Jul 1; 115 (4): 599-605. - Montella M, Maso LD, Crispo A, Talamini R, Bidoli E, Grimaldi M, Giudice A, Pinto A, Franceschi S. Do childhood diseases affect NHL and HL risk? A case-control study from northern and southern Italy. Leuk Res. 2006 Aug; 30 (8): 917-22.
- Shaheenet SO, Aaby P, Hall AJ, Barker DJ, Heyes CB, Shiell AW, Goudiaby A. Measles and atopy in Guinea-Bissau. Lancet. 1996 Jun 29; 347: 1792-6.
- Rosenlund H, Bergström A, Alm JS, Swartz J, Scheynius A, van Hage M, Johansen K, Brunekreef B, von Mutius E, Ege MJ, Riedler J, Braun-Fahrländer C, Waser M, Pershagen G; PARSIFAL Study Group. Allergic disease and atopic sensitization in children in relation to measles vaccination and measles infection. Pediatrics. 2009 Mar; 123 (3): 771-8.
- Kubota Y, Iso H, Tamakoshi A, JACC Study Group. Association of measles and mumps with cardiovascular disease. The Japan Collaborative Cohort (JACC) study. Atherosclerosis. 2015 August; 241 (2): 682-6.
- Waaijenborg S, Hahné SJ, Mollema L, Smits GP, Berbers GA, van der Klis FR, de Melker HE, Wallinga J. Waning of maternal antibodies against measles, mumps, rubella, and varicella in communities with contrasting vaccination coverage. J Infect Dis. 2013 Jul; 208 (1): 10-6.
- Poland GA, Jacobson RM. The re-emergence of measles in developed countries: time to develop the next-generation measles vaccines? Vaccine. 2012 Jan 5; 30 (2): 103-4.
- Physicians for Informed Consent. Measles - vaccine risk statement (VRS). Dec 2017. https://www.physiciansforinformedconsent.org/measles/vrs.
- Demicheli V, Rivetti A, Debalini MG, Di Pietrantonj C. Vaccines for measles, mumps and rubella in children. Cochrane Database of Syst Rev. 2012 Feb 15; (2).
- 10 leading causes of death by age group, United States — 2015. Atlanta: Centers for Disease Control and Prevention [cited 2017 June 21]. https://www.cdc.gov/injury/images/lc-charts/leading_causes_of_death_age_group_2015_1050w740h.gif.
- US Department of Health, Education, and Welfare. Vital statistics of the United States 1962, volume 2 — mortality, part A. Washington DC: US Government Printing Office; 1964. 94.
{kind=link}
Source: https://physiciansforinformedconsent.org/wp-content/uploads/2019/06/PIC-Measles-DIS-Italian.pdf